The Federal Picture: Why Cardiovascular Adults Are Paying Attention to Infrared Saunas
Start with the number that matters most: cardiovascular disease accounts for approximately 1 in 3 U.S. deaths annually, according to CDC WONDER mortality tracking. That is not a rounded estimate — it is the most precisely tracked cause-of-death figure in federal public health. For a condition responsible for one-third of American deaths, any evidence-based adjunct intervention attracts attention. Infrared sauna use is one of those adjuncts, and the federal data trail around it is more substantive than most wellness coverage suggests.
At the same time, passive heat therapy is not a drug. It is not a substitute for medication management, physician-guided cardiac rehabilitation, or — most critically — aerobic physical activity. The CDC's Behavioral Risk Factor Surveillance System (BRFSS) documents that approximately 76% of U.S. adults do not meet the 150-minutes-per-week moderate aerobic activity guideline, a gap that directly compounds cardiovascular and inflammatory burden. Any honest evaluation of infrared sauna use has to begin there: the evidence base for saunas is strongest in populations who are also physically active. Passive heat is an adjunct, not a workaround.
With that framing established, this article does something most sauna coverage does not: it maps what federal agencies — CDC, NIOSH, FDA, and AHRQ — actually document about thermal therapy, explains the mechanism, and only then discusses products.
Who This Article Is For
This article is written specifically for adults with diagnosed or elevated-risk cardiovascular conditions — including hypertension, coronary artery disease, heart failure in remission, and metabolic syndrome — who are researching whether infrared sauna use can be a meaningful part of a broader cardiovascular health strategy. It is also written for workers in physically demanding occupations (construction, agriculture, manufacturing, healthcare) where the NIOSH Total Worker Health framework explicitly integrates recovery interventions, including thermal therapy, as part of comprehensive occupational health — not separate wellness.
If you have a clinical cardiac history, this article is informational analysis of federal data, not medical advice. Every section that touches on contraindications will tell you plainly: clear this with your cardiologist first.
Why Thermal Physiology Is Relevant to Cardiovascular Adaptation
To understand why federal research has taken passive heat therapy seriously, you need to understand the mechanism — not as marketed by a sauna brand, but as described in physiology research that NIOSH and federal agencies have indexed.
When core body temperature rises, even passively, the cardiovascular system responds in ways that partially mimic moderate aerobic exercise. Heart rate increases — typically 50 to 75% above resting in a Finnish-style sauna session. Peripheral blood vessels dilate to dissipate heat, reducing vascular resistance. Cardiac output rises. Sweat gland activity activates. The result is a transient hemodynamic load that, with repeated exposure, has been associated in observational cohorts with measurable adaptations: lower resting blood pressure, improved endothelial function, reduced arterial stiffness.
NIOSH-cited research documents that passive heat therapy interventions, including sauna use, are associated with measurable cardiovascular and circulatory adaptation in regular users. The key word is "regular" — single sessions produce transient effects; the associations with cardiovascular outcomes in the literature come from cohorts using saunas four to seven times per week over years. This is a frequency most Americans are not approaching with a gym membership, let alone a home sauna.
Infrared saunas operate at lower ambient temperatures (typically 120–150°F versus 170–195°F in traditional Finnish saunas) using near-, mid-, or far-infrared wavelengths that penetrate skin tissue directly. This produces similar core temperature elevation with a subjectively more tolerable environment — relevant for cardiovascular patients who may not tolerate high ambient heat well. The lower-temperature environment is also part of why FDA has reviewed infrared therapy devices under its 510(k) Class II clearance pathway, which indexes manufacturer safety claims and provides federal-level review that traditional sauna products have not historically undergone.
The CDC PLACES dataset tracks cardiovascular disease, hypertension, and stroke rates at the county level — the exact conditions represented in the strongest sauna-benefit research. That granularity matters: the counties with highest cardiovascular burden often overlap with high physical-demand occupational concentrations, which is precisely the demographic NIOSH's Total Worker Health program addresses.
The Inflammatory Burden Dimension
Cardiovascular disease does not exist in isolation. CDC arthritis data shows that approximately 25% of U.S. adults report doctor-diagnosed arthritis, with concentration in occupations involving sustained physical demand — the same occupational populations with elevated cardiovascular risk. Inflammatory arthritis and cardiovascular disease share a systemic inflammatory pathway (elevated CRP, IL-6, TNF-alpha), and both have been studied in the context of heat therapy's potential anti-inflammatory effects. For the cardiovascular-health reader who also manages arthritis or inflammatory pain, this overlap is clinically meaningful — sauna research on inflammatory markers is part of the same federal data context.
AHRQ Medical Expenditure Panel Survey (MEPS) data further contextualizes why preventive intervention research matters: adults with chronic cardiovascular conditions face substantially higher annual healthcare costs than cardiovascular-healthy adults. The cost differential motivates serious research interest in whether low-cost adjunct interventions — including thermal therapy — can reduce disease progression and utilization downstream.
The Safety Architecture: What Federal Agencies Flag
Before discussing what saunas may do for cardiovascular health, the honest data journalism question is: what does the federal safety record look like?
The FDA Adverse Event Reporting System (FAERS) provides federal-level safety data on adverse events associated with thermal therapy devices. The FAERS record for infrared devices is not alarming at population scale, but adverse events do occur — primarily in users who ignore contraindications. The major risk profile is hemodynamic: rapid peripheral vasodilation combined with dehydration can cause orthostatic hypotension (blood pressure drop on standing), syncope, and — in high-risk cardiac patients — arrhythmia provocation.
This is not a reason to avoid saunas. It is a reason to approach them correctly. The interventions below address exactly this safety architecture before you consider any equipment purchase.
Try These First — Free Interventions Before Any Equipment Purchase
The most important principle in occupational and preventive health: the cheapest intervention is the one that does not require buying anything. The following are evidence-anchored behavioral protocols that federal agencies and NIH specifically document. They are not optional add-ons to sauna use — for cardiovascular-health readers, they are prerequisites.
Hydration before and after is the single most actionable free intervention. A 20-minute sauna session can produce 0.5 to 1 liter of sweat loss. CDC NIOSH heat-stress guidance translates directly: pre-hydrate with at least 16 oz of water before a session, and replace fluid plus electrolytes within an hour of exit. For cardiovascular patients on diuretics — a common medication class — electrolyte monitoring is especially relevant, because sweat-driven losses compound drug-induced losses.
Pair sauna with light cardio for circulation. The most cited cardiovascular benefit data from sauna research comes from cohorts who also met CDC physical activity guidelines — 150 minutes of moderate aerobic activity per week. Sauna is not a cardiovascular exercise substitute. It is a complement that may amplify recovery and circulatory adaptation in people who are already physically active. If you are among the 76% of adults not meeting activity guidelines, addressing that gap first is the higher-yield intervention.
Clear heat therapy with a clinician before starting. NIH NCCIH guidance on sauna use explicitly flags uncontrolled hypertension, recent cardiac events, pregnancy, and medications affecting thermoregulation as conditions requiring physician clearance before heat therapy. This is not boilerplate — it is a specific clinical signal.
Time sessions for sleep compatibility. NIH sleep guidance is clear: core body temperature must drop to initiate sleep onset. Using a sauna immediately before bed delays that drop. Finish your last heat session at least 90 minutes before lights-out so core temperature can normalize.
Avoid sauna during pregnancy. CDC pregnancy guidance and NIH cohort data consistently advise against sauna use during pregnancy — elevated maternal core temperature in the first trimester is associated with neural tube defects in multiple cohort studies.
If you have already adopted these protocols, are physically active, have received clinical clearance, and are looking for equipment that fits your cardiovascular health goals, then products become a rational next consideration. Not before. The rest of this article evaluates specific options through that lens.
When to See a Clinician: Red Flags Specific to Cardiovascular Users
For the cardiovascular-health audience specifically, certain signals should stop a sauna session immediately and prompt medical evaluation — not next-day, immediately. Federal guidance is explicit on the following:
Uncontrolled hypertension (systolic consistently above 180 mmHg or diastolic above 120 mmHg) is a hard contraindication according to NIH NCCIH sauna guidance. The vasodilatory response of heat therapy can cause rapid, unpredictable blood pressure swings in uncontrolled hypertensives. If your blood pressure control has changed recently — new medication, dosage adjustment, lifestyle disruption — reestablish stability before resuming sessions.
Recent cardiac events — myocardial infarction, unstable angina, decompensated heart failure, significant arrhythmia — require a physician's explicit sign-off before any heat therapy. The hemodynamic demands of a sauna session are not trivial for a recently stressed heart. Most cardiac rehabilitation programs have protocols for when heat therapy can be reintroduced; your cardiologist can map this to your specific history.
If you experience chest discomfort, palpitations, unusual shortness of breath, presyncope (lightheadedness), or visual disturbance during a session: exit immediately, cool down gradually, hydrate, and seek evaluation. The FDA FAERS adverse event record for infrared devices clusters around these exact presentations in users who did not observe contraindications. These are not statistical abstractions — they are the documented pattern.
Where Products Fit: Equipment That Serves the Cardiovascular-Health Protocol
With mechanism, free interventions, and clinical red flags established, equipment evaluation becomes a question of fit for the specific use case: frequency, space, budget, and — critically for cardiovascular users — the ability to control temperature precisely and safely.
For cardiovascular-health users, the most important product attributes are not luxury features. They are: consistent, controllable low-to-moderate heat output; EMF-shielded or low-EMF panels (reducing ancillary radiation exposure during extended use); precise digital temperature control; and build quality sufficient to maintain consistent performance across the four-to-seven-sessions-per-week frequency that the research cohorts actually used.
The Almost Heaven Pinnacle 4-Person Barrel Sauna is the outdoor barrel sauna pick for this reader — not because of its aesthetic, but because its thermal mass and traditional-style design produce consistent, sustained heat exposure that maps to the Finnish cohort data most referenced in cardiovascular research. At $5,499, it is a durable, outdoor-first installation that makes daily or near-daily sessions a structural part of your routine rather than a friction-laden production. The barrel geometry efficiently retains heat with less energy input, and the 4-person capacity is generous enough for a full-recline session if mobility is a factor. For cardiovascular-health users who want a long-term, outdoor sauna practice anchored in the frequency patterns that the research actually documents, this is the structural investment to evaluate.
For readers for whom $5,499 is not feasible, or who rent, travel, or lack outdoor installation space, the HigherDOSE Infrared Sauna Blanket V4 at $599 offers a portable, full-body far-infrared exposure format. The Blanket V4 uses far-infrared technology — the wavelength range most associated with deep tissue penetration and the circulatory response — and is FDA-reviewed under the 510(k) pathway relevant to this article's safety context. It produces the core temperature elevation that drives the hemodynamic response in a format that is accessible regardless of living situation. Clinical note: the blanket format requires the same hydration, timing, and contraindication protocols as any other infrared modality. Convenience does not reduce clinical responsibility.
For cardiovascular-health users evaluating these options: the research cohorts were not using equipment casually. They were using it regularly, at appropriate temperatures, in combination with physical activity and good hydration practices. Equipment quality matters because inconsistent heat output means inconsistent sessions, and inconsistent sessions break the frequency pattern the evidence base actually requires.
Infrared Saunas Evaluated for Cardiovascular-Health Users
These products were selected specifically for adults managing cardiovascular risk who need consistent, controllable heat exposure for regular therapeutic use — not occasional spa recreation.
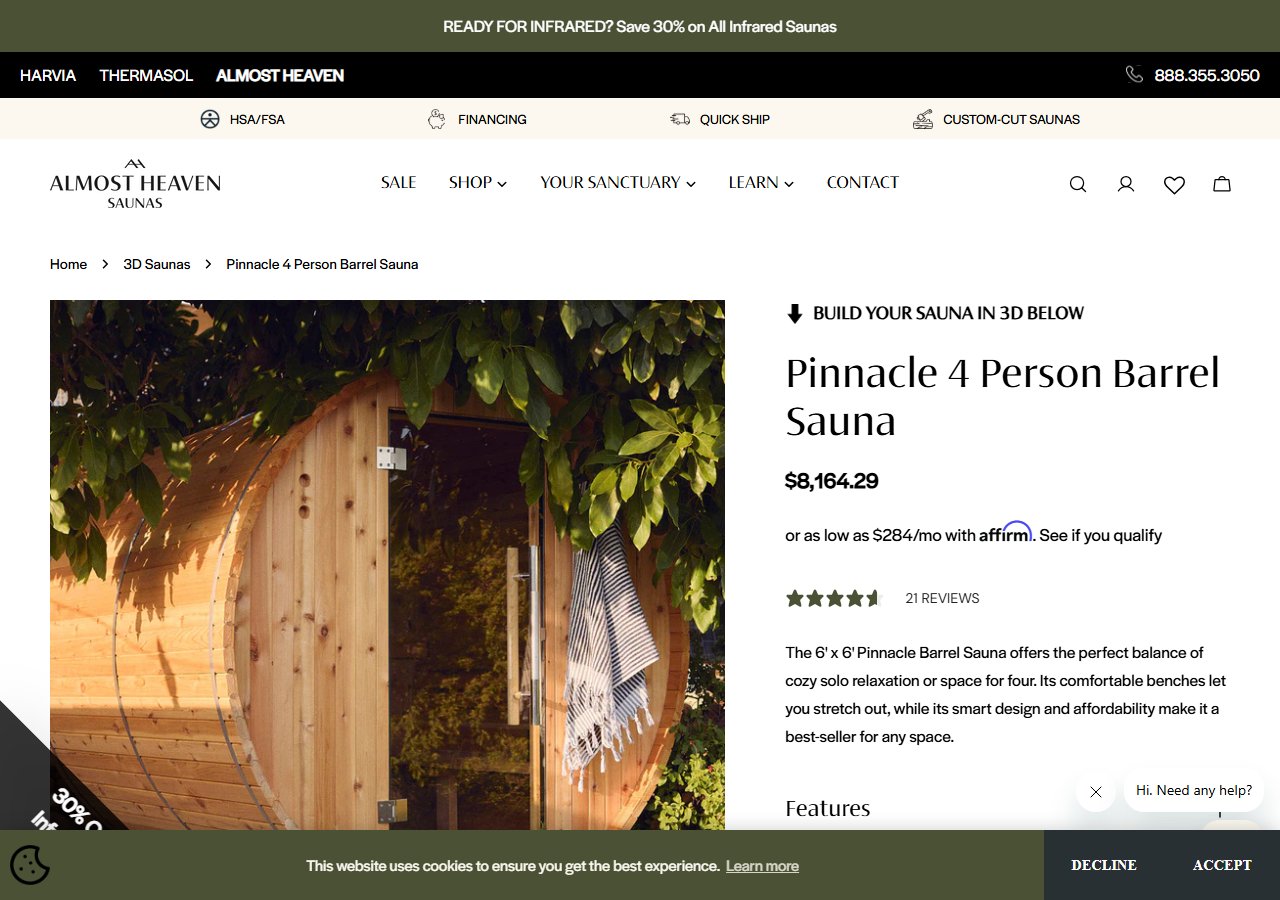
Almost Heaven Pinnacle 4-Person Barrel Sauna
$5,499
See Price at Almost Heaven →
HigherDOSE Infrared Sauna Blanket V4
$599
See Price at HigherDOSE →Synthesizing the Federal Data Picture
Let's close by returning to what the data actually supports — not what sauna marketing claims.
Cardiovascular disease kills 1 in 3 Americans annually per CDC WONDER. That mortality burden is what makes any evidence-based adjunct intervention worth serious evaluation. Federal research — indexed through NIOSH, analyzed in context of CDC PLACES cardiovascular county data, and reviewed for safety through the FDA 510(k) and FAERS systems — documents that passive heat therapy is associated with cardiovascular and circulatory adaptation in regular users. The operative words: associated, regular, users who are also physically active.
The AHRQ MEPS cost data makes the preventive logic compelling: cardiovascular disease is extraordinarily expensive downstream. If passive heat therapy contributes meaningfully to blood pressure management, arterial flexibility, and inflammatory burden reduction — in combination with exercise, medication adherence, and clinical management — the long-term cost-benefit picture for the right user is defensible.
The NIOSH Total Worker Health framework explicitly integrates thermal therapy into comprehensive occupational health for physically demanding workers. That federal framing matters: this is not fringe wellness. It is federally-contextualized recovery science.
But the hierarchy is non-negotiable: activity guidelines first, clinical clearance first, hydration protocols first, correct timing first — and only then, equipment. The 76% of American adults not meeting aerobic activity guidelines will not recover that cardiovascular gap with a sauna. The adults who have addressed those fundamentals and are looking for a disciplined, evidence-anchored adjunct have a defensible case for infrared sauna integration into their cardiovascular health protocol.
The evidence supports that case. Federal data sets the boundaries. Your cardiologist closes the loop.